Cardiology Blog
Be sure to check back regularly for the latest in cardiovascular care along the Gulf Coast, informative posts about heart health, and more.
Renal Denervation for High Blood Pressure: What Gulf Coast Patients Need to Know
Think of renal denervation as a way to "quiet down" overactive nerves near the kidneys that are making blood pressure too high. Both Dr. John Galla and Dr. Stan Thornton were the first to locally treat patients at Springhill Medical Center and Thomas Hospital, respectively, using the minimally invasive treatment at and FDA-approved Medtronic Symplicity Spyral™ Renal Denervation System. Offering new hope for patients in the area with high blood pressure that is uncontrolled or unresponsive to medication.
The Problem with Hard-to-Control Blood Pressure
High blood pressure affects nearly one in two American adults. But here's the scary part — only about one in five people who have it has it under control. For many patients, taking blood pressure medicine every day still isn't enough. Their numbers stay dangerously high, which raises their risk for stroke, heart attack, kidney failure, and heart disease.
For a long time, there wasn't much else doctors could offer these patients. That changed in 2024, when the FDA approved a new procedure called **renal denervation (RDN)**. It's the only non-drug treatment for high blood pressure that the FDA has ever approved. Here in Southwest Alabama and along the Gulf Coast, Cardiology Associates is one of the first practices to offer it.
What Is Renal Denervation?
Think of renal denervation as a way to "quiet down" overactive nerves near the kidneys that are making blood pressure too high.
Here's how it works: Your kidneys help control blood pressure by sending signals through nerves to your brain. In some people, those nerves are way too active. They keep sending signals that push blood pressure up — even when you're taking medicine to bring it down.
During renal denervation, a doctor uses a thin, flexible tube called a catheter. It goes in through a small opening at the wrist or groin and is guided to the arteries near the kidneys. Then, gentle energy (called radiofrequency energy) is used to calm down those overactive nerves.
The procedure usually takes less than an hour. You don't need to be put completely to sleep, and most patients go home the same day. The goal isn't to replace your blood pressure medicine — it's to help your medicine (and your body) work better.
Does It Work? What the Research Shows
Yes — and there's strong evidence to back it up.
Cardiology Associates uses the Medtronic Symplicity Spyral™ system. It has been tested in several large, carefully designed studies.
One combined analysis showed that renal denervation cut the chances of a dangerous blood pressure emergency by 43%. That's a big deal for patients who have been struggling for years to get their numbers down.
Major heart organizations in Europe now recommend renal denervation as an add-on treatment for patients with hard-to-control high blood pressure.
Cardiology Associates: Leaders in Renal Denervation on the Gulf Coast
Cardiology Associates has been caring for patients in Mobile and Baldwin County for decades. Two of our doctors are leading the way when it comes to renal denervation in this region.
Dr. John Galla, MD, FACC, FSCAI — Mobile, Alabama
Dr. John Galla is an interventional cardiologist at Cardiology Associates in Mobile, Alabama. He trained at two of the top programs in the country — Duke University for his residency and the Cleveland Clinic for his coronary and interventional cardiology training.
He is an experienced cardiologist and focuses on treating blockages, heart valve problems, and hard-to-control blood pressure.
Dr. Stan Thornton, MD, FACC, FSCAI — Fairhope, Alabama
Dr. Stan Thornton is an interventional cardiologist at Cardiology Associates in Fairhope, Alabama. He trained at Oschner Clinic Foundation for both his interventional and cardiovascular diseases fellowships. He is a Principal Investigator for the U.S. portion of a major worldwide study called the Global Symplicity Registry DEFINE — or GSR-DEFINE.
In a historic moment, Dr. Thornton treated the very first patient enrolled in the U.S. part of the Global SYMPLICITY Registry (GSR) DEFINE clinical trial. This study is tracking up to 5,000 patients across 251 hospitals in 55 countries to see how renal denervation works in real-world practice. The fact that the first U.S. patient was treated right here on the Gulf Coast shows just how much trust the medical community places in Dr. Thornton and Cardiology Associates.
A Track Record of Firsts
Both Dr. Galla and Dr. Thornton were the first to locally treat patients at Springhill Medical Center and Thomas Hospital, respectively, using the minimally invasive treatment at and FDA-approved Medtronic Symplicity Spyral™ Renal Denervation System. Offering new hope for patients in the area with high blood pressure that is uncontrolled or unresponsive to medication.
Could Renal Denervation Be Right for You?
This procedure isn't for everyone. But you might be a good candidate if:
Your blood pressure is still high even though you take one or more blood pressure medicine
You have bad side effects from blood pressure medicines and can't take them well
You've been taking your medicine the right way but still can't get your numbers under control
Your doctor has checked and your kidney arteries are a good fit for the procedure
Some people — such as those with certain types of kidney disease or blood pressure caused by another medical problem — may not be good candidates. Your doctor will do a full checkup before recommending this procedure.
What to Expect
Before the procedure: Your doctor will look at your blood pressure history and your medicines. You'll likely wear a blood pressure monitor for 24 hours to get a clear picture of your readings throughout the day and night.
During the procedure: It is performed in the catheterization lab in the hospital. You'll get medicine to help you relax, but you won't be fully put to sleep. A thin tube is guided to the arteries near your kidneys, and gentle energy is used to calm the overactive nerves. It takes about 30 to 60 minutes.
After the procedure: Most patients rest for a few hours and then go home. There's no large incision, nothing left inside your body, and no long recovery period.
Follow-up: Your doctor will track your blood pressure in the weeks and months after the procedure. Your medicines may be adjusted as your body responds.
Why Choose Cardiology Associates?
Experienced doctors. Dr. Galla and Dr. Thornton were among the first in the region to offer renal denervation.
Full heart care. Renal denervation is just one piece of the puzzle. Our team looks at your whole heart and vascular health and builds a plan that fits you.
Close to home. With offices in Mobile, Fairhope and Foley, we serve patients across the Alabama, Mississippi and Florida Gulf Coast.
Ready to Learn More?
If your blood pressure has been hard to control — or if you're tired of taking multiple medications without seeing results — it may be time to ask about renal denervation.
Consult your primary care physician or call Cardiology Associates to arrange a visit with Dr. John Galla in Mobile or Dr. Stan Thornton in Fairhope. We'll go over your health history, answer your questions, and help you decide if this treatment is a good fit.
Cardiology Associates | Serving Mobile and Baldwin County, Alabama and surrounding communities. Offices in Mobile, Fairhope, and Foley
Carotid Stent: A Less Invasive Option to Treat Carotid Artery Disease and Help Lower Stroke Risk
Learn about the minimally invasive procedure to treat carotid artery disease, how it works, and whether it might be right for you — and what to expect before and after treatment for carotid artery disease.
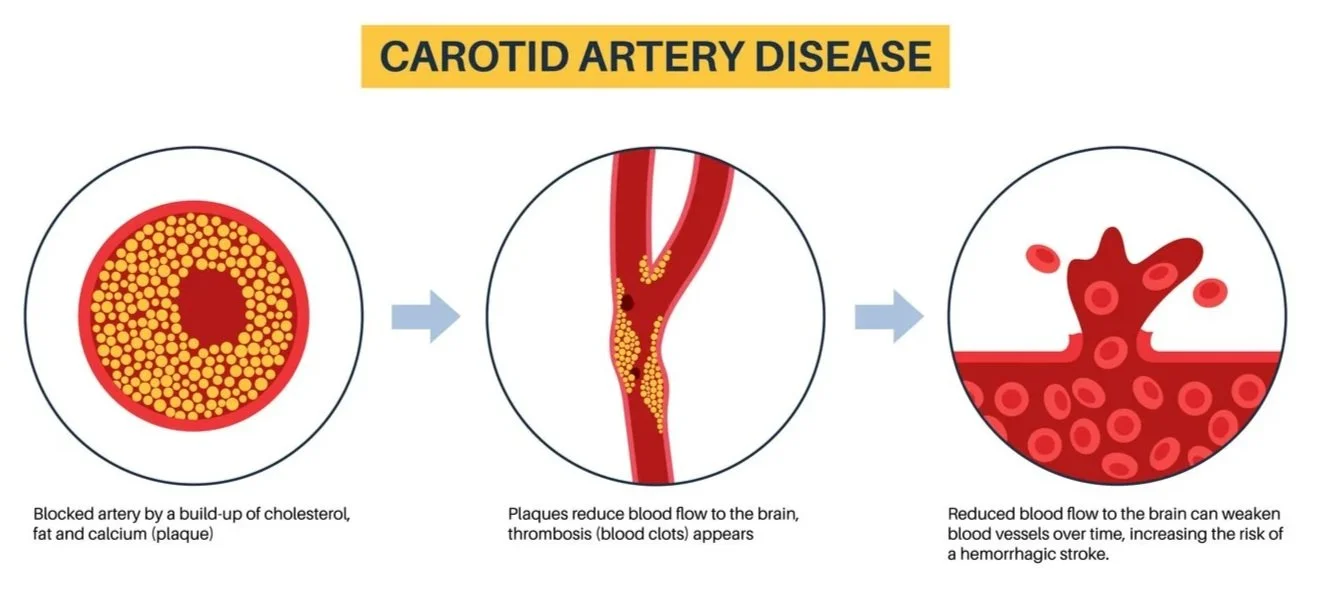
The carotid arteries are major blood vessels in the neck that supply oxygen-rich blood to the brain. When these arteries become narrowed due to plaque buildup, the condition is known as carotid artery disease, or carotid stenosis. This narrowing can restrict blood flow to the brain and significantly increase the risk of stroke.
For some patients, carotid angioplasty may be a recommended treatment option. This minimally invasive procedure is used to assess the extent of narrowing and to open a blocked or narrowed carotid artery.
What is carotid stenting?
Carotid stenting is a minimally invasive procedure, like a heart catheterization, used to treat significant narrowing in a carotid artery. During the procedure, a physician guides a thin tube called a catheter through the blood vessels to the narrowed area. A small balloon may be used to open the artery, and a metal mesh tube called a stent is placed to help keep the artery open. A filter is often used during the procedure to catch debris and help lower the chance of plaque traveling to the brain.
Why does carotid artery disease matter?
When plaque builds up in the carotid arteries, it can increase the risk of stroke or transient ischemic attack (TIA), sometimes called a “mini stroke.” Some patients have symptoms, and others may have no warning signs at all before the disease is found in imaging or during an evaluation.
Possible warning signs of stroke or TIA can include, and require immediate attention:
Sudden weakness or numbness on one side of the body
Trouble speaking or understanding speech
Sudden vision changes
Dizziness or loss of balance
Sudden and severe headache
Who may be a candidate for carotid stenting?
Carotid stenting is not right for every patient. Treatment decisions, for patients with carotid artery disease, will depend on how severe the narrowing is, whether the patient has had stroke or TIA symptoms, overall health, and the anatomy of the artery. In some cases, carotid stenting may be chosen instead of carotid surgery based on patient-specific factors and the care team’s evaluation.
Benefits of a less invasive approach
Because carotid stenting is a catheter-based treatment, it may be a good option for selected patients who need treatment but may not be ideal candidates for traditional surgery. It is designed to improve blood flow through the artery while avoiding a larger surgical incision.
What happens during the procedure?
During carotid stenting, a cardiologist threads a catheter through the blood vessels to the narrowed carotid artery. A protection device may be placed to catch loose plaque during the procedure. The narrowed area is opened, and the stent is positioned to act as a scaffold and help keep the artery from narrowing again.
What to expect after a carotid stent procedure?
After the procedure, patients are monitored closely by their care team. Recovery instructions may include guidance about activity, medications, and follow-up visits. Even after a stent is placed, ongoing treatment remains important, including control of blood pressure, cholesterol, diabetes, and smoking cessation when needed.
Expert cardiac and vascular care close to home
At Cardiology Associates, in Mobile, Fairhope and Foley, Alabama, our cardiologists evaluate patients with vascular disease and help determine the most appropriate treatment plan based on each patient’s condition and overall health. If carotid artery disease is found, early evaluation and treatment planning can play an important role in reducing stroke risk.
When to talk with your cardiologist
You should speak with your physician if you have been told you have carotid artery narrowing, have had a stroke or TIA, or have risk factors such as high blood pressure, high cholesterol, diabetes, or smoking history. A full evaluation can help determine whether medical therapy, surgery, or carotid stenting may be the best next step.
With timely diagnosis and expert care, patients with carotid artery disease may have more options to help protect brain health and reduce stroke risk.
To learn more or request an appointment with Cardiology Associates, call 251-607-9797 or visit: https://www.cardassoc.com/procedures or https://www.cardassoc.com/john-m-galla
TAVR: A Less Invasive Option for Treating Severe Aortic Stenosis
TAVR, a minimally invasive procedure, used to treat severe aortic stenosis. Because TAVR is less invasive than traditional surgery, many patients may benefit from smaller incisions, a shorter hospital stay and faster recovery. For appropriate patients, TAVR can help relieve symptoms and improve quality of life.
When the aortic valve becomes narrowed or calcified, the heart must work harder to pump blood to the body. This condition is called aortic stenosis. It is one of the most serious and common heart valve problems, and when symptoms become severe, valve replacement is often needed.
For some patients, a less invasive treatment option is TAVR, which stands for transcatheter aortic valve replacement. TAVR replaces the damaged aortic valve by guiding a new valve to the heart through a catheter, usually through a blood vessel in the groin, rather than through traditional open-heart surgery.
What is TAVR?
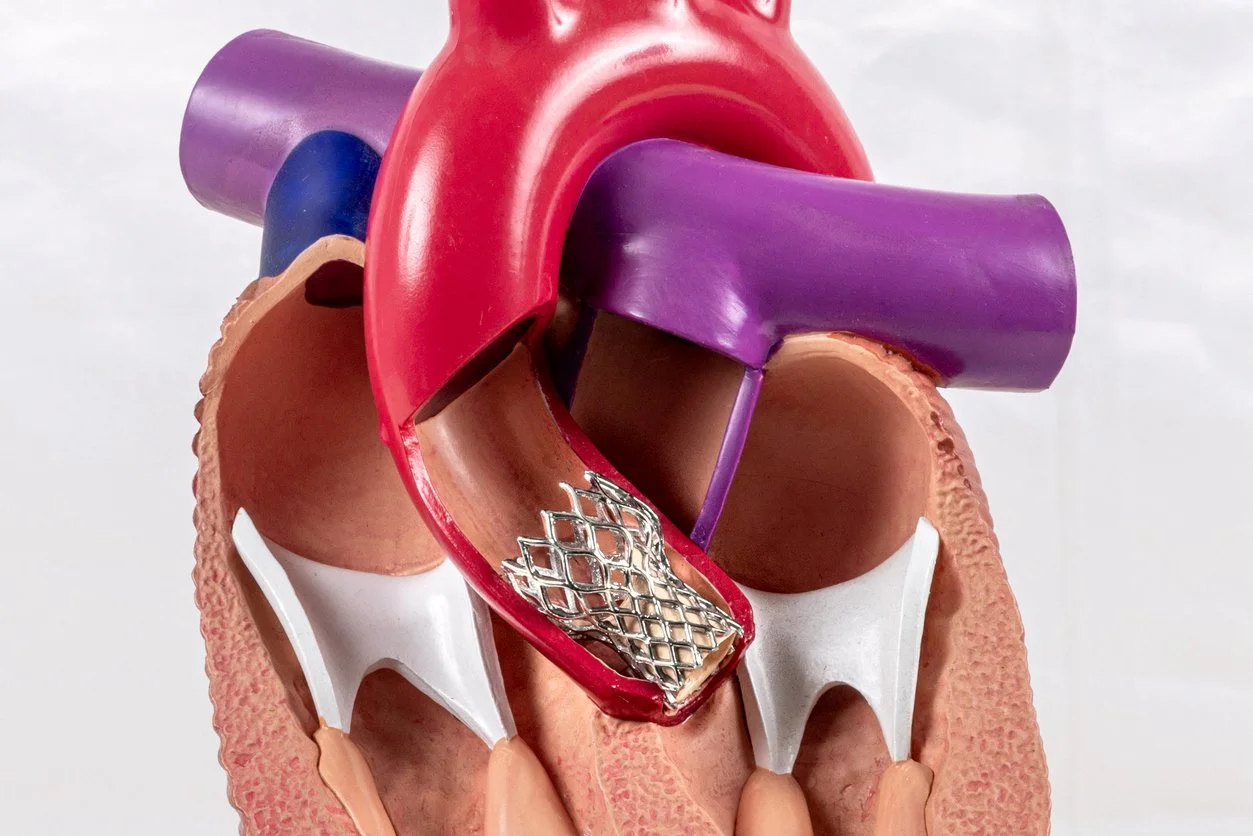
TAVR is a minimally invasive procedure used to treat severe aortic stenosis, a condition in which the leaflets of aortic valve become calcified, or stenotic, and the valve does not open the way it should. During the procedure, a replacement valve is placed inside the diseased valve. Once expanded, the new valve takes over the job of regulating blood flow from the heart to the rest of the body.
Signs and symptoms of aortic stenosis
Aortic stenosis can reduce blood flow and place extra strain on the heart. Symptoms may include shortness of breath, chest pain, fatigue, dizziness, or fainting. Some people may not notice symptoms until the condition becomes more advanced.
Who may be a candidate for TAVR?
TAVR may be an option for patients with symptomatic severe aortic stenosis. Cardiology Associates structural team collaborates and evaluates each patient carefully to determine whether TAVR, surgical valve replacement, or another treatment is the best choice. That evaluation will include imaging, testing, and a review of the patient’s overall health, symptoms, and treatment goals.
Benefits of a less invasive approach
Because TAVR is less invasive than traditional surgery, many patients may benefit from smaller incisions, a shorter hospital stay, and a faster recovery. For appropriate patients, TAVR can help relieve symptoms and improve quality of life.
What happens during the procedure?
During TAVR, the interventional cardiologist guides a catheter through a blood vessel to the heart and positions the new valve inside the diseased aortic valve. The replacement valve is then expanded, pushing the old valve leaflets aside and allowing blood to move more normally through the heart.
What to expect after TAVR
After the procedure, patients are monitored closely by their structural heart care team. Recovery instructions vary, some patients can go home the same day, others may need an overnight stay. Follow-up visits are important to make sure the new valve is working properly and healing is progressing as expected. Patients will be given information about activity, medications, and ongoing care before going home.
Expert heart valve care close to home
The structural heart team at Cardiology Associates provides evaluation and treatment for patients with advanced valve disease, including severe aortic stenosis. We work closely with patients and families to determine the right treatment plan and offer experienced, comprehensive heart care close to home.
Cardiology Associates was the first to perform TAVR in Mobile Alabama in 2011, soon after the procedure received FDA approval. Our team includes the most experienced structural heart specialists in on the Gulf Coast, helping patients access advanced treatment options in the communities we serve.
When to talk with a cardiologist
If you have been told you have aortic stenosis or are experiencing symptoms such as shortness of breath, chest discomfort, fatigue, or fainting, it is important to seek evaluation. Early diagnosis and expert assessment can help determine whether TAVR or another treatment may be right for you.
To learn more or request an appointment , call 251-340-6852 or visit https://www.cardassoc.com/structural-heart

Your Heart Beat Can Tell On You
Afib or Atrial Fibrillation is a common condition affecting the heart’s beat, rhythm and rate that many people hear about and that is becoming more common.
Pacemaker and Defibrillator Basics by Jordan M. Chiasson, MD, FACC Cardiac Electrophysiologist
Afib or Atrial Fibrillation is a common condition affecting the heart’s beat, rhythm and rate that many people hear about and that is becoming more common. By the year 2050 it is predicted that it will affect between 6-12 million Americans. Afib is the most common type of an irregular heart beat that if left untreated can cause complications, even stroke. An electrophysiologist is a cardiologist specializing in the heart’s circuitry system and addresses issues with the timing on one’s heartbeat.
There are numerous types of technology, medications and monitoring systems to assist patients in addressing complications when the heart’s electrical system is disturbed and can make significant life changing improvements.
Pacemakers and defibrillators regulate the heart’s rate & rhythm. following are some frequently asked questions and answers.
1. What is a pacemaker?
A pacemaker is an electronic device made up of a battery or “pulse generator” connected to one or more wires or “leads” that monitors and regulates the heart rate and rhythm. There are several different types of pacemakers, and they work by stimulating the heart or “pacing” it with electrical impulses programmed to restore a normal heartbeat.
2. What is the difference between a pacemaker and a defibrillator?
A defibrillator is composed of a thicker lead and larger battery. In addition to being able to pace the heart, defibrillators have advanced monitoring and treatment capabilities if dangerous or life-threatening rhythms are detected. Defibrillators are generally reserved for patients with a diagnosis of congestive heart failure or those who have survived a cardiac arrest.
3. How are these devices implanted?
In the electrophysiology laboratory, similar to a cardiac catheterization laboratory, the leads are inserted into the axillary or subclavian vein, which is the main route from the arm or shoulder to the heart. The leads are then positioned under X-ray guidance and tested to be sure they will function properly. Next the leads are attached to the battery, which is tucked into a small pocket created under the skin. The incision is generally no more than 1-2 inches long and is closed with dissolving stitches.
4. What’s new with pacemakers and defibrillators these days?
Leadless pacemakers are now commercially available and are widely used to treat certain rhythm disorders. These devices are about the size of a paperclip or vitamin, and do not require an incision or pocket. Ask your doctor if this is the right type of pacemaker for you.
In addition, new implantation techniques are emerging that can allow pacemakers and defibrillators to better simulate the heart’s normal electrical conduction. There is ongoing research to determine if this is better for the heart over the long term, and early data has shown promising results.
5. I have a pacemaker or a defibrillator, what happens next?
The device will need to be periodically checked or “interrogated” to be sure it is programmed appropriately and individually optimized. This can often be done remotely, or from home, with the aid of a trans-telephonic monitor. The pulse generators are usually powered by lithium batteries that function for an average of 5-8 years before they need to be replaced.
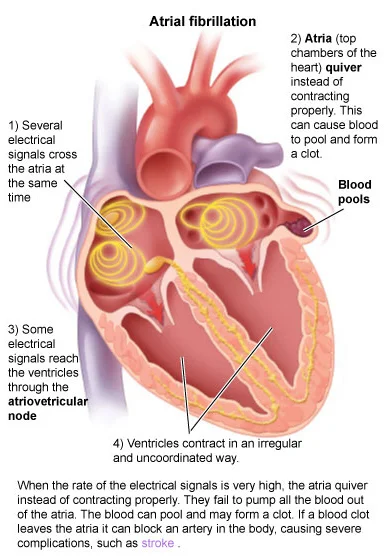
What is Atrial Fibrillation, Afib ?
Atrial fibrillation is a complex arrhythmia (abnormal heart rhythm) affecting the upper chambers of the heart (the atria) primarily. During atrial fibrillation, the atria beat very rapidly (over 300 beats per minute), and much of the pumping activity of this portion of the heart is lost. Additionally it drives the main pumping chambers of the heart (the ventricles) rapidly, and while the ventricles are unable to go as fast as the atria, pulse rates over 150 beats per minute are not uncommon.
By Dr. Matthew Quin, Cardiac Electrophysiologist
Atrial fibrillation is a complex arrhythmia (abnormal heart rhythm) affecting the upper chambers of the heart (the atria) primarily. During atrial fibrillation, the atria beat very rapidly (over 300 beats per minute), and much of the pumping activity of this portion of the heart is lost. Additionally it drives the main pumping chambers of the heart (the ventricles) rapidly, and while the ventricles are unable to go as fast as the atria, pulse rates over 150 beats per minute are not uncommon.
What causes atrial fibrillation?
Atrial fibrillation usually does not have one single factor underlying the disease, although there are some instances where this is true (such as high thyroid levels). In most individuals, atrial fibrillation is a result of an inherited tendency (to some degree) as well as other factors; conditions such as high blood pressure, obesity or overweight, obstructive sleep apnea, diabetes mellitus, coronary heart disease, or heart failure are often associated with the development of atrial fibrillation. Depending on an individual's symptoms, each of these is assessed as part of the evaluation of atrial fibrillation.
What are the symptoms of atrial fibrillation?
In a minority of people, atrial fibrillation has no symptoms at all. However, many people adjust their level of activity in such a way as to minimize symptoms--these individuals restructure their activity to accommodate the disease. In most people, atrial fibrillation does lead to symptoms--most commonly fatigue, shortness of breath, a sensation of rapid heart beat, or chest pain. Occasionally symptoms such as lightheadedness (or rarely fainting) can be attributed to atrial fibrillation as well. These symptoms are largely related to the rapid heart beat caused by atrial fibrillation as well as the reduced pumping capability of the heart when atrial fibrillation starts.
There are other concerns beyond the symptoms associated with atrial fibrillation however; atrial fibrillation is one of the most common causes for strokes as well as heart failure. Because of the reduced pumping capability of the heart, blood tends to pool in small channels naturally located along the inside of the heart; when blood pools, it tends to form clots. If these blood clots then break free and escape into the blood stream then they can cause strokes if the blood clot goes to the brain. Blood clots going to other organs can lead to problems at those locations as well--even problems such as kidney disease and heart attacks. In addition to the risk of stroke, the rapid heart rates associated with atrial fibrillation can lead to heart failure, or a condition called "tachycardia-mediated cardiomyopathy". Reduction in the heart rate (and treatment of the underlying atrial fibrillation) is key in treating this condition.
What can be done about atrial fibrillation?
After evaluation for underlying conditions which may contribute to the development of atrial fibrillation, attention is focused on therapy. There are a variety of therapies available for atrial fibrillation, with the best therapy personalized for the symptoms, age and lifestyle of the individual. In some people, medications called anti-arrhythmic drugs are an effective means of suppression of atrial fibrillation. Some benefit from a simple procedure called a cardioversion, which is a shock administered to the heart to stop the abnormal rhythm and allow the body's normal rhythm to resume. In select individuals, atrial fibrillation can be treated directly with a procedure performed within the heart called an ablation, during which the triggers for atrial fibrillation are directly targeted and destroyed or isolated with a heated wire called a catheter. And finally, for some people a pacemaker provides a good option for control of symptoms related to atrial fibrillation; while a pacemaker does not eliminate atrial fibrillation, it can ameliorate many of the associated symptoms.
What is the long term prognosis?
With good medical care, atrial fibrillation is a condition that individuals live with, not die from. But ongoing therapy is important to prevent the complications mentioned above, but also because atrial fibrillation is associated with other adverse health outcomes such as dementia. Adherence to medications along with routine follow up with your physician is important for maintaining your health.

Facts About Cardiac Calcium Screening
Cardiology Associates has offered Cardiac Calcium Screening since 2005 and has experience in conducting thousands of these tests. It is a tremendous tool in helping to predict and treat patients with cardiac conditions.
Cardiology Associates has been involved with Cardiac Calcium Screening for over 18 years and have experience in conducting thousands of these tests. It is a tremendous tool in helping to predict and treat patients with cardiac conditions.
What is Cardiac Calcium Screening?
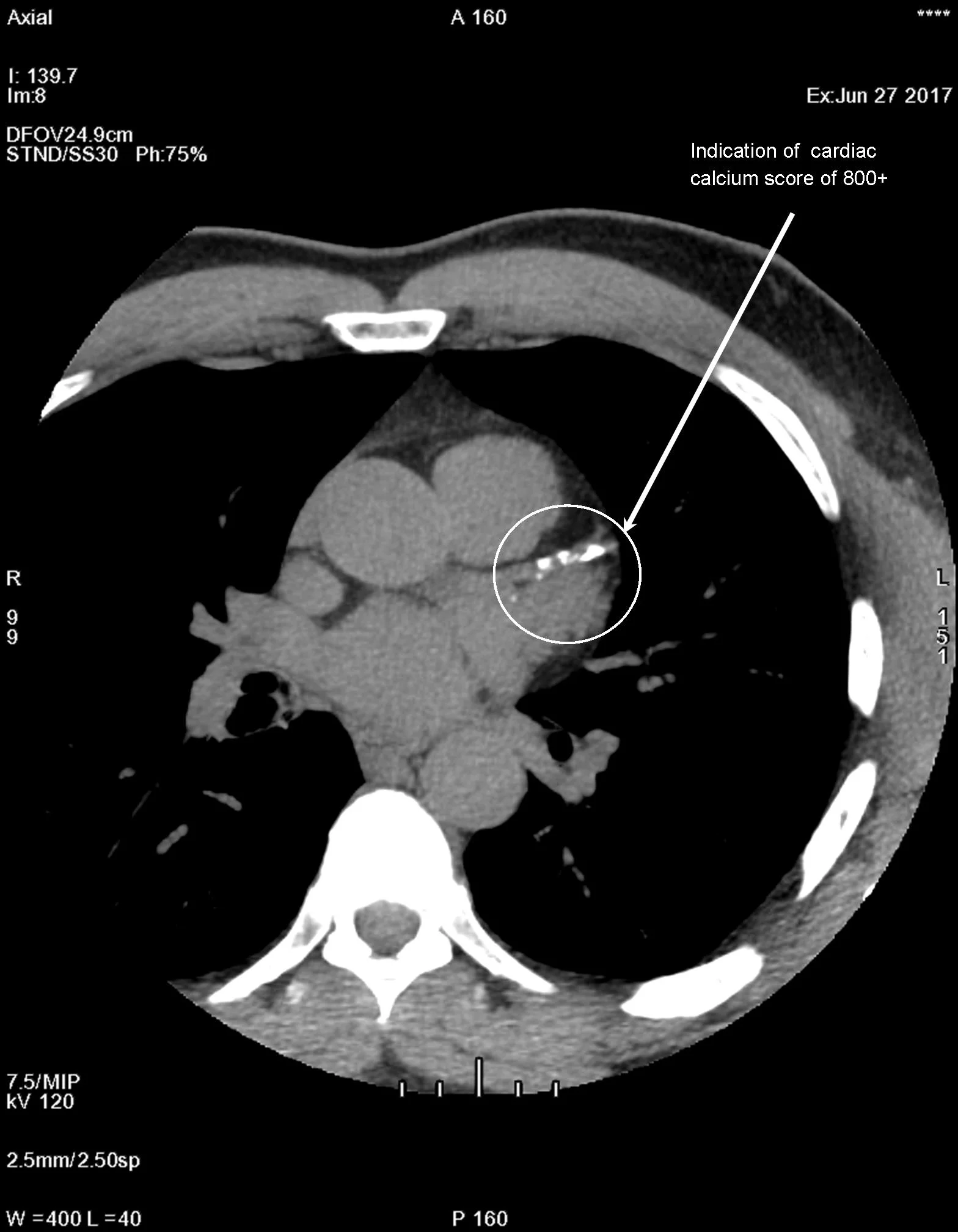
This is a screening test performed on our ultra-fast CT scanner that measures how much calcified plaque is present in the heart arteries. Today’s research shows a direct correlation between the amount of calcium in these arteries and the likelihood of future cardiac events such as a heart attack or stroke. It is an overall assessment of one’s global risk for heart disease. The amount and density of the calcified plaque can predict the likelihood of a cardiac event, such as heart attack or need for coronary intervention over the next one to two years of the screening.
Who is an appropriate candidate to have a Cardiac Calcium Screening test?
If you have not had any symptoms and have any of the following you may consider having this screening. If you have a family history of heart disease, high cholesterol, high triglycerides, low HDL, high blood pressure, diabetes, overweight, inactive or are a male over 45 years of age or a woman over 55 years of age.
We offer Cardiac Calcium Screenings at our offices in Mobile on the campus of Springhill Medical Center and in Fairhope on the campus of Thomas Hospital.
How is the plaque measured if present?
A calcium score is compared to a national database and analyzed against other patients of the same age and gender. The following is what is used in defining your level of risk for developing coronary artery disease.
Score of 0 – No evidence of plaque and less than a 5% chance you have CAD
Score of 1-10 – Risk for heart attack is low, small amount of plaque is present. Consider quitting smoking, improving diet and getting regular exercise.
Score of 11-100 – Risk for heart attack is moderate. Plaque is present, CAD is present but only mild hardening of the arteries.
Score of 101-400 – Risk for heart attack is moderate to high. Plaque is present in moderate amount, CAD is present and plaque may be blocking an artery. Physician may suggest additional testing.
Score of 400+ - Risk for heart attack is high. Plaque is present and extensive. More than a 90% chance plaque is blocking one of the coronary arteries. Physician will recommend additional testing.
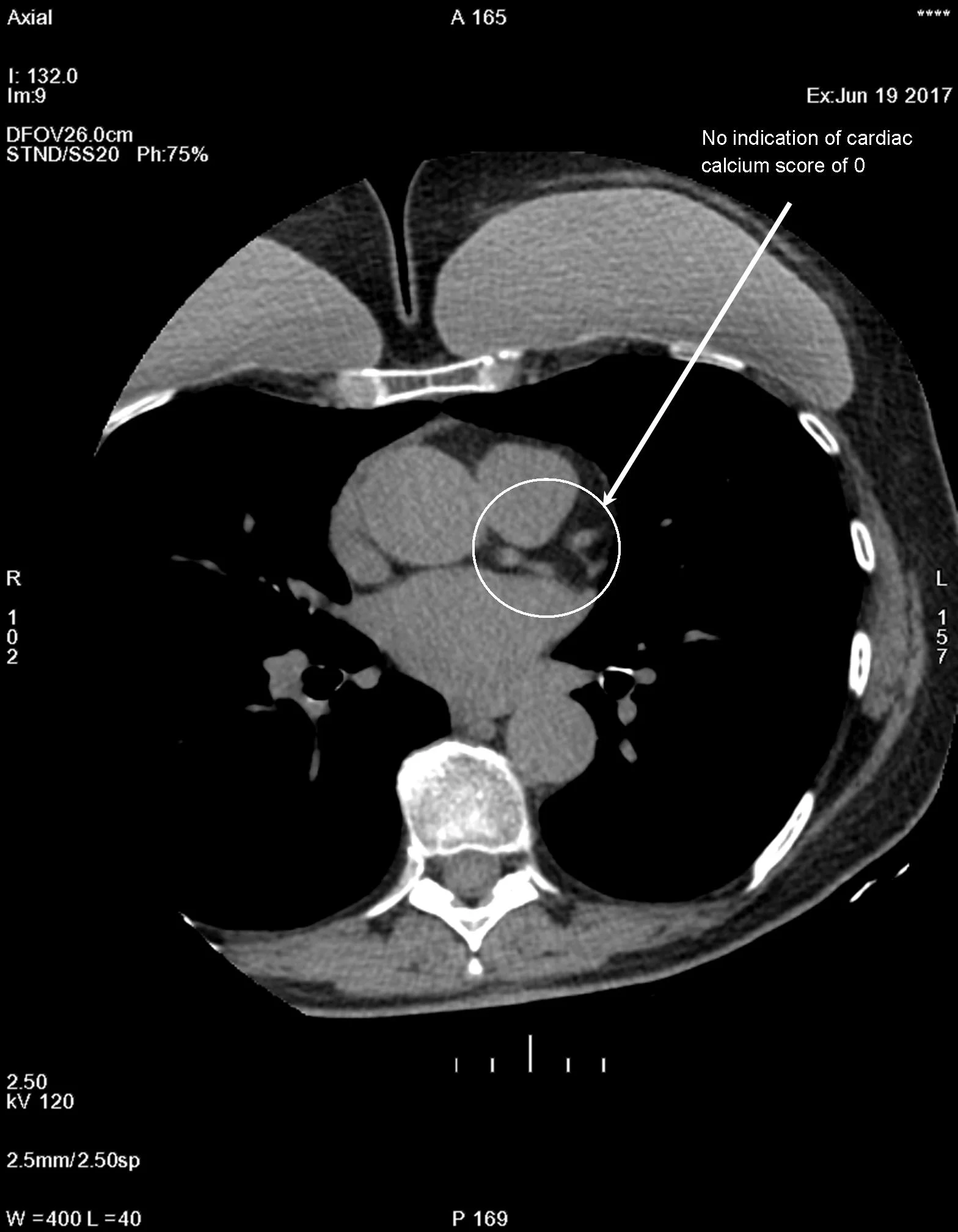
Cardiac calcium score images from an ultra-fast CT of the heart. Photo to the left no plaque is present, with a score of zero. Photo on the right plaque is present, with a score of 802.